Home
Home Patient Login
Patient Login International patients
International patients Contact Us
Contact Us Emergency
Emergency Download Reports
Download Reports

Patient Stories & Experiences


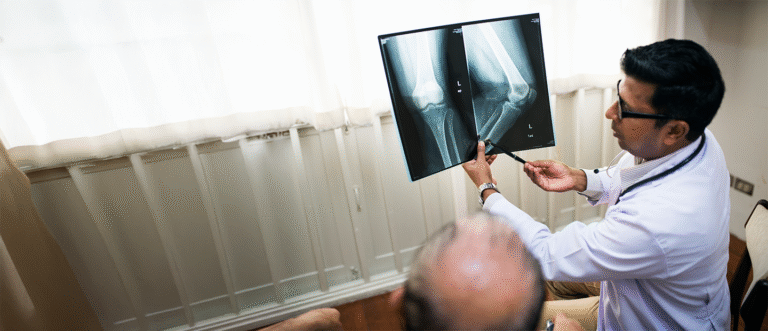
The pain in my left knee left me feeling helpless for years. After my treatment here, I can finally say I'm pain-free.
Vinita Singh

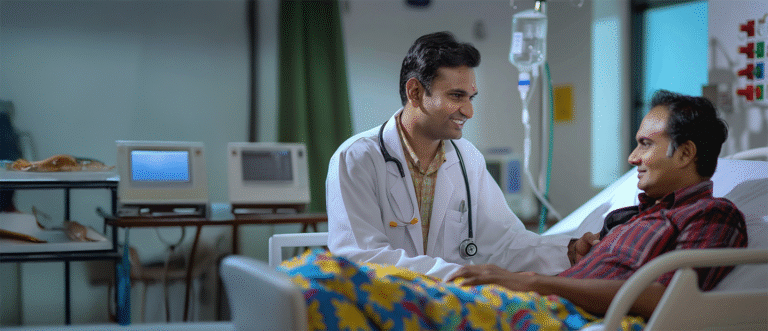
The nerves were swollen, and the body went numb. But thanks to Sancheti Hospital, I got a second life!
Parvati

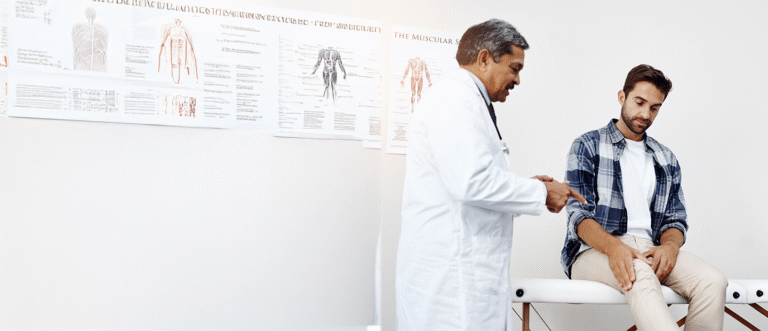
I finally could walk again, a relief I've only felt after the hip pain surgery. I thank the doctors at Sancheti Hospital for their help.
Balaji Kharat

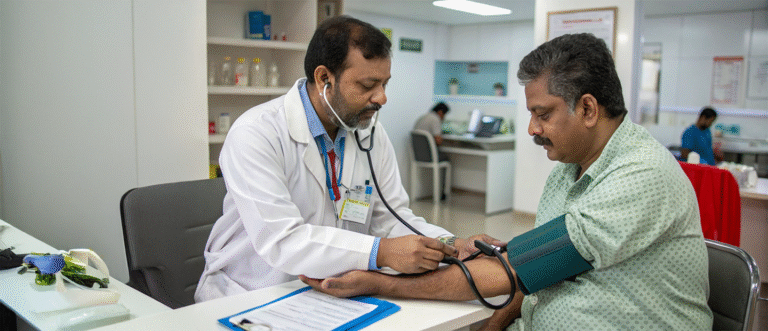
I'm a police officer, and I'm extremely thankful to Sancheti Hospital for treating my fracture without surgery.
Shantilal

My life has completely changed after the knee replacement surgery at Sancheti Hospital. It's like I can finally live again!
Kalpana Lepcha

The knee pain I've carried for years finally went away with the help of Sancheti Hospital.
Karuna

I can't believe that I get to finally live a normal and happy life, all thanks to the knee surgery I had at Sancheti Hospital.
Kishore Bhosle